(NEW YORK) — Over the last several years, cases of valley fever, a disease common to the arid West, have been steadily creeping up.
Between 2014 and 2018, valley fever cases tripled in California alone, and the state reached a record high of 9,004 new cases in 2019.
Now, experts believe the disease may spread to other parts of the country, and it may be due to climate change.
“I have talked to some people that the cases are over the usual numbers,” Dr. George Thompson, a professor of medicine at UC Davis, said. “We’re probably up 30% [in my practice].”
Valley fever, or coccidioidomycosis, is caused by the coccidioides fungus and can manifest as a primarily respiratory illness that self-resolves, or as a more severe, systemic condition that requires immediate medical attention.
The more severe version, disseminated coccidioidomycosis, affects 5-10% of infected people and can affect the skin, joints, heart and even the brain and spinal cord. Once those areas are impacted, the disease can be difficult to treat, particularly in immunocompromised individuals.
The coccidioides fungal spores commonly reside in soil throughout California, Arizona, Nevada, New Mexico, Utah, Texas and as far north as Washington. Any disturbance of the dirt, such as construction work and burrowing animals, can send plumes of coccidiodes spores into the air, where people can inhale them.
While valley fever is historically endemic to the hot and dry southwestern United States, experts are concerned that the fungus may be on the move due to ecologic and environmental changes, among other factors.
“There’s a bit of seasonality … it’s multifactorial. There’s no question there’s been a strong, steady increase,” Dr. Andrew Comrie, a professor of climatology at the University of Arizona, told ABC News.
Improved surveillance and diagnostic methods may be catching more valley fever cases than before, but experts believe the recent rise in known cases is, in some part, a result of changing global climate trends.
So far, research based on predictive modeling has shown that changing climate patterns may lead to coccidioides spreading as far east as Kansas and as far north as North Dakota.
These models are based on trends seen in precipitation and temperature: two factors critical to the lifecycle of the fungus responsible for valley fever.
Projections show that average annual temperature may increase by 3-6 degrees by the end of the 21st century, and rainfall is predicted to decrease further in the western and southwestern U.S. — setting up more ideal environments for coccidiodes to spread.
But climate change might not be wholly to blame for the fungus’ spread.
“It’s a lot hazier than we would like it to be,” Comrie said.
Predictive modeling can only provide part of the story based on estimates, and there is inherently a time lag between when a patient is diagnosed with valley fever and when that person was actually exposed to the fungus.
Comrie also pointed out other theories, debunking one myth in particular, which sets duststorms as the enemy. Duststorms — gigantic walls of loose dirt — commonly blow through Arizona, and people may worry that toxic fungal spores are released in the air along with the dust. However, Comrie wants to dispel that fear (overall, Valley fever appears uncorrelated with duststorms as a whole) and instead focus on rodents as potential vectors for valley fever. Burrowing mice, for example, easily disturb the soil layer where the coccidiodes fungi sit, increasing the risk of dissipating the dangerous spores.
“More disturbances means more infections,” Comrie said, which in turn means more attention needs to be given to valley fever, as experts believe it will only become more common in the country as the environment changes.
“A lot of primary care doctors are going to be the first ones to encounter the disease,” Thompson said. “It’s important for patients to know whether they need to get tested for coccidiodes.”
(WASHINGTON) — An independent Food and Drug Administration advisory panel on Thursday voted unanimously to authorize Moderna Covid-19 vaccine boosters for Americans 65 and older, anyone 18 and older with underlying conditions and those frequently exposed to the virus.
The recommendation is in line with what the FDA and Centers for Disease Control and Prevention authorized for Pfizer booster shots last month.
The Moderna booster will only be a half dose, as opposed to the full dose for Pfizer, but was found to return antibody protection to the initial levels after the first two shots.
Dr. Jacqueline Miller, who presented Moderna’s data Thursday, said the company chose the half dose because it was just as effective but would “increase the worldwide vaccine supply of mRNA.”
Moderna and the FDA both said there was no evidence of increased side effects from booster doses except for more reports of swelling or tenderness in the arm where the patient was injected.
“Unsolicited adverse events did not reflect any new safety concerns,” the FDA found.
On Friday, the panel will also vote on authorizing booster shots for the third available vaccine, Johnson & Johnson. Johnson & Johnson posted a summary of its research Wednesday, making the argument for a second shot of the same dose, roughly six months after the initial single-shot vaccine.
The conversation around boosters focuses on whether Americans vaccinated over six months ago need a boost of protection against breakthrough infections in the face of the more transmissible delta variant, though all of the three vaccines authorized in the U.S. are still proving effective against hospitalization and death.
And despite the overwhelming support for boosters from the experts on the FDA panel, many were also quick to point out that the conversation around boosters should not undermine the vital campaign to get the 66 million unvaccinated Americans vaccinated.
“The people who are in the ICU aren’t there because they haven’t gotten the third dose, they’re there because they haven’t gotten any dose,” Dr. Paul Offit, an FDA advisory panel member and director of the Vaccine Education Center at Children’s Hospital of Philadelphia, said in Thursday’s meeting.
Another panel member, Dr. Michael Kurilla of the National Institute of Health, noted that the vaccines are still working quite well, particularly among young people, and he doesn’t see the need to offer boosters universally.
“I don’t necessarily see the need for a sort of let-it-rip campaign for boosters for everyone who’s ever been vaccinated,” Kurilla said.
Another pertinent debate that the FDA panel will take on Friday is the potential benefits of mixing and matching vaccines for booster shots.
Early results from a highly anticipated National Institutes of Health study found that boosting with a shot different from what people got the first time appears to be safe and effective.
The non-peer reviewed study evaluated all three vaccines — Pfizer, Moderna and J&J — finding that no matter the booster, all study participants saw a “substantial” uptick in antibody levels after a booster shot.
Though promising, more research is likely needed on mixing and matching. For now, the process will formally move forward with authorizing additional booster doses of Moderna and Johnson & Johnson shots for those who received the same original vaccine.
This week’s meetings are the first step in that process: The FDA itself and the Centers for Disease Control and Prevention will both need to sign off on the panel’s recommendations about who should get boosters and when for Moderna and J&J.
The first authorization, which will come from the FDA, is expected within days of the independent panel’s non-binding vote.
Then, the question goes to CDC’s independent advisory panel of experts. That panel has scheduled a meeting for next Wednesday and Thursday to discuss boosters for Moderna and Johnson & Johnson. Those outside experts will weigh in with their recommendations, which are also non-binding.
Once that happens, CDC Director Rochelle Walensky must sign off, which typically happens within 24 hours of the panel’s recommendations. That decision is expected by Friday, Oct. 22, at the earliest.
(NEW YORK) — When a Wyoming coroner announced Tuesday that Gabby Petito, the 22-year-old travel blogger whose remains were recovered in September in a national park, died by strangulation, experts who study intimate partner violence said they saw a recognizable thread.
“Strangulation is not talked about as much, but it is a major risk factor for intimate partner homicide,” Kellie Lynch, an associate professor at the University of Texas at San Antonio, told Good Morning America. “And we often see it occur alongside more severe abuse.”
“When you’re talking about strangulation, that is very typically the cause of death in domestic violence cases,” Dan Abrams, ABC News chief legal analyst, said in an interview Wednesday on GMA. “It is angry. It is violent. It takes time. That is precisely what many believe happened here.”
Petito’s death was ruled a homicide and the cause is officially listed as “manual strangulation/throttling,” according to the coroner.
Petito’s boyfriend and cross-country traveling companion, Brian Laundrie, has been named by investigators as a person of interest in her death and is the subject of a massive nationwide search being directed by the FBI.
While the search continues for Laundrie, he’s also wanted on charges of bank fraud for allegedly using Petito’s credit card. Experts said the case has shined a spotlight on intimate partner violence and the many forms it can take.
Strangulation is one of the most lethal forms of domestic violence, one that can cause death within minutes, according to the National Domestic Violence Hotline, a 24/7, free and confidential resource.
It is also a predictor for future deadly violence, experts said. A non-fatal strangling in the past by a partner makes the victim 10 times more likely to be killed by them later on, according to the National Domestic Violence Hotline.
“I think people are now starting to appreciate the seriousness of strangulation, both that it’s more frequent than we realize and also that it can be more lethal than we realize,” Kiersten Stewart, director of public policy and advocacy of Futures Without Violence, a nonprofit organization focused on ending violence against women and children, told GMA. “When we train health care providers, strangulation is one of the very specific issues that we talk about to help them recognize it.”
Symptoms of strangulation can range from a sore throat and difficulty swallowing to bruising, memory loss, difficulty breathing and changes in sleep, mood and personality, among others, according to the National Domestic Violence Hotline.
Strangulation in cases of intimate partner violence is often about control, and in non-fatal cases, it may not leave as evident of a mark as other forms of physical abuse, experts said.
Stewart and other experts note that when cases like Petito’s are in the news, though extremely tragic, they can raise awareness about intimate partner violence and the many different forms it may take.
“Domestic violence is still a very serious issue,” said Stewart, noting young people between the ages of 18 and 24 experience the highest rates of domestic violence. “As a country, we have made great progress in the last 25 years, but we haven’t actually reduced homicides nearly as dramatically, and that still needs to be a real focus.”
In his eulogy at his daughter’s funeral last month, Joseph Petito referenced the issue, telling mourners, “If there is a relationship that you’re in that might not be the best thing for you, leave it now. Take care of yourself first.”
Intimate partner violence, which falls under the broader umbrella term of domestic violence, affects more than 12 million people every year, and disproportionately impacts Black and Indigenous women, according to the National Domestic Violence Hotline. It has historically been seen by many as something that happens with older, married couples, or something that involves only physical abuse, like a black eye, the organization said.
In reality, it is something that cuts across all social and demographic lines and can also occur through control and manipulation that is not as easily visible to the outside world, according to Lynch.
“We have these myths or stereotypes in our head of a typical domestic violence abuser and victim, who they are and what they act like, but everybody is at risk,” she said. “People would be very surprised to find out just how prevalent it is and how many people they know who’ve experienced it at some point.”
While acknowledging that not all details of the incident are known, both Lynch and Stewart pointed to body camera footage of Petito and Laundrie being pulled over in Arches National Park in Utah in August after a report of an alleged domestic problem.
The footage showed Petito, who appeared to be crying, at one point sitting in the back of a police vehicle, and Laundrie, at other points, talking to police officers.
Petito told police she suffers from severe anxiety and other medical conditions and that the couple’s argument had been building for days. Police labeled the incident as a “mental/emotional break” rather than a domestic assault, according to the police report.
“I don’t know how much we’re going to know about the relationship and the dynamic between the two of them, but in the video, she seemed frightened and scared,” Lynch said of Petito. “I think across all of these cases [of intimate partner violence], that’s what you’re going to see, someone is intimidated.”
Stewart said she sees in the video fear from Petito, which she calls a red flag.
“You can’t always tell the first time you meet somebody what’s going on,” she said. “But once you’ve started to have a conversation, if you see somebody who’s very much afraid, like, ‘If I were to not do what he wants, what happens?’ that’s often a red flag.”
Abuse in relationships, which data shows is more often, but not always, perpetrated by men, comes down to “power and control,” according to Rosemary Estrada-Rade, director of quality assurance and innovation at the National Domestic Violence Hotline.
“It’s about that pattern of behaviors that are used within relationships to maintain that control over the other partner,” she said. “So it could be physical violence, but a lot of times it’s intimidation, manipulation, emotional abuse, financial abuse and financial control, and that can look different in different relationships.”
Signs that someone may be suffering from intimate partner violence include isolation from family and friends, appearing withdrawn or not like themselves, frequent calls or texts from their partner about where they are and who they’re with and other controlling behaviors, like withholding money or restricting a person’s ability to work, according to Estrada-Rade.
When a case like Petito’s is in the headlines, it can help draw awareness to the issue of intimate partner violence and increase education, experts said.
In Sarasota, Florida, around 30 miles from the town where police say Laundrie was last seen, calls to a local domestic violence shelter have increased 15% over the past month, compared to the same time last year. The shelter’s CEO attributes the increase to both the pandemic and headlines around the Petito case.
“Domestic violence is something that people shy away from, they don’t want to talk about it,” Jessica Hays, president and CEO of Safe Place and Rape Crisis Center in Sarasota, told “GMA.” “I think that anytime that we have an opportunity to talk about how common domestic violence is, and the warning signs and just shine a light on the fact that this is something that affects many, many people and is not the fault of the victim and that there is help and support out there, that’s a really important conversation.”
The National Domestic Violence Hotline has experienced a 46% increase in contacts in the past five years, according to a spokeswoman, who also attributed the yearslong increase in calls to a combination of factors.
“While we can’t say definitively that seeing or hearing about reports of abuse or domestic violence in the media causes an increase in contacts, we do know that news reports and even depictions of tactics of power and control in other media can help survivors recognize that they might be experiencing abuse and that they can reach out to us,” the spokeswoman said.
Experts said that is the most important takeaway, the recognition that there is help out there for everyone touched by intimate partner violence, from those experiencing it to those committing it to those trying to help.
“During this Domestic Violence Awareness Month, we really are encouraging those who feel that they may be in an abusive or controlling relationship to get help, to talk to somebody,” said Stewart. “And also, we really encourage people who may be using violence in their relationships to also reach out for help because that’s really the behavior we need to change.”
If you need help or need help supporting someone else, call the National Domestic Violence Hotline at 1-800-799-7233, or go to thehotline.org. All calls are toll-free and confidential. The hotline is available 24/7 in more than 170 languages.
(WASHINGTON) — An independent FDA advisory panel on Thursday and Friday is set to discuss and vote on whether to authorize Moderna and Johnson & Johnson Covid-19 vaccine boosters for those 18 and older.
The outside experts will also consider new data from the National Institutes of Health on the potential benefits of mixing and matching vaccines for booster shots.
Early results from the highly anticipated NIH study finds that boosting with a shot different from what people got the first time appears to be safe and effective.
The non-peer reviewed study evaluated all three vaccines — Pfizer, Moderna and J&J — finding that no matter the booster, all study participants saw a “substantial” uptick in antibody levels after a booster shot.
Though promising, more research is likely needed on mixing and matching. For now, the FDA and CDC are slated to weigh in on whether to authorize additional booster doses of Moderna and Johnson & Johnson shots for those who received the same original vaccine.
This week’s meetings are the first step in a long process: The FDA itself and the Centers for Disease Control and Prevention would both need to sign off on the panel’s recommendations about who should get boosters and when — and the earliest that could happen is the following Friday, Oct. 22.
On Thursday, the panel will discuss and vote on a potential Moderna booster, and hear presentations from both the company and FDA representatives; Israel’s director of public health health will give a presentation about the results of Pfizer booster shots in that country.
The FDA panel will ask questions and debate the benefits versus risks of a Moderna booster and an initial, non-binding vote on the Moderna booster has been scheduled for Thursday afternoon.
On Friday, the panel will discuss and vote on a Johnson & Johnson booster, in addition to hearing NIH’s presentation on mix and match booster data.
Johnson & Johnson’s posted a summary of its research Wednesday, making the argument for a second shot, same dose, roughly six months after the single-shot vaccine.
An initial, non-binding vote on the Johnson & Johnson booster has been scheduled for Friday afternoon.
Once the FDA advisory panel votes on recommendations for each booster, the FDA itself needs to formally amend the current emergency authorization. FDA career scientists are expected to authorize boosters for Johnson & Johnson and Moderna within days of the independent panel’s non-binding vote.
Then, the question goes to CDC’s independent advisory panel of experts. That panel has scheduled a meeting for next Wednesday Oct. 20 and Thursday Oct. 21 to discuss boosters for Moderna and Johnson & Johnson. Those outside experts will weigh in with their recommendations, which are also non-binding.
Once that happens, CDC Director Rochelle Walensky must sign off, which typically happens within 24 hours of the panel’s recommendations.
(NEW YORK) — Despite more than 187 million Americans being fully vaccinated against COVID-19 and data and attestations from researchers and public health officials that the vaccines are safe an effective, a small and in some cases vocal minority of Americans are reluctant to get the shot.
The reasons vary, but a number of those people are instead turning to treatments after they are diagnosed that have far less evidence to support their safety and effectiveness, including monoclonal antibodies — a trend that experts say is worrying.
Currently, over 1 million doses of monoclonal antibody infusions have been given in the United States. Use of monoclonal antibodies gained steam during the delta variant surge over the summer when Florida and other states opened clinics to administer the drugs in an attempt to keep sick people out of overwhelmed hospitals.
Monoclonal antibodies have been authorized for post-exposure prophylaxis, meaning they are used shortly after someone tests positive in order to prevent progression to severe disease. The antibodies range in effectiveness depending on type, but some have been shown in to reduce COVID-related hospitalization or death by up to 85%.
COVID-19 vaccines have been tested in large clinical trials with hundreds of thousands of people. The CDC says over 215 million people have safely received at least one dose of a COVID-19 vaccine, including 187 million who have been fully vaccinated, either with the one-dose Johnson & Johnson shot, or two dose mRNA vaccines.
All three COVID-19 vaccines have gone through the most intensive safety monitoring in U.S. history by government agencies, fully independent safety monitoring boards, vaccine manufacturers and academic researchers. The Pfizer COVID vaccine is currently FDA authorized for people 12 and older. The Moderna and Johnson & Johnson vaccines are authorized for those 18 and up.
Common side effects of the COVID-19 vaccine include pain or swelling at the injection site. Fever, muscle aches, chills, fatigue or headaches can also occur but should go away within a few days. More serious health problems, such as unusual heart rhythm or blood clots, are exceedingly rare — and in fact, are more likely to happen to an unvaccinated person who becomes sick with COVID-19 than with the vaccine itself.
‘More concerned with treatment rather than prevention’
Many vaccine holdouts in the U.S. have cited the vaccines’ emergency use authorization status — a special FDA pathway helps accelerate the often-slow regulatory process during a national emergency. Pfizer’s vaccine is now fully FDA approved for people 16 and older, while Moderna and Johnson & Johnson are still under emergency authorization, awaiting approval.
However, some experts interviewed by ABC news say some patients who won’t get vaccinated also ask for monoclonal antibody treatment after the are diagnosed with COVID, which has the same emergency use authorization. Doctors say they are perplexed about why some people pursue monoclonal antibody treatment which is supposed to reduce the risk of hospitalization in high-risk vulnerable people instead of prevention.
“People are more concerned with treatment rather than prevention,” said Rupali Limaye, Ph.D., the director of behavioral and implementation science for the International Vaccine Access Center at Johns Hopkins School of Public Health.
“When they are in the hospital and needing COVID treatment, their options are limited — but they know they need treatment to fight COVID. Decision-making is very different related to preventative behaviors,” said Limaye.
What to know about monoclonal antibodies
The FDA has granted emergency authorization status to four antibody treatments for COVID-19. These antibody treatments are most helpful in mild to moderate disease. Not all antibody treatments are equally effective, and some have lost their potency in the face of new COVID-19 variants.
According to the FDA, monoclonal antibodies are laboratory-made proteins designed to mimic the immune system’s ability to fight disease particles known as antigens. For example, sotrovimab is a monoclonal antibody that prevents COVID-19 infection by blocking the virus’ spike protein.
The data supporting these antibodies is much more limited than the extensive data supporting currently approved and authorized vaccines.
“Monoclonal antibodies are an important treatment option for high-risk patients. However, the idea that they can be used as a prevention tool is severely misguided,” said Dr. Andrew Pavia, Infectious Diseases Society of America fellow, NIH COVID treatment guidelines panel member and chief of pediatric infectious diseases at the University of Utah School of Medicine.
“They are no substitute for cheap and effective prevention tools like masks and vaccines,” said Pavia.
Other COVID treatments under EUA include tocilizumab, a monoclonal antibody that is not directed toward the virus but instead reduces inflammation in already hospitalized patients. Remdesivir, an anti-viral, is FDA approved for hospitalized patients over 12 but under EUA for kids less than 12.
All of these treatments require an infusion and a trip to a medical center. Now, pharmaceutical companies are also working on easy-to-prescribe pills that can ease symptoms for people who are already sick, but doctors stress these are also not a replacement for a vaccine that can help prevent disease in the first place.
Ways to boost vaccination
Doctors interviewed by ABC News say their patients want an easy solution that will protect them from COVID-19. For most, that’s a vaccine. For others, misinformation surrounding vaccines can stand in the way, prompting them to seek alternatives.
“Hesitancy falls on a continuum. That means that those that are hesitant may refuse some vaccines, may accept vaccines but be unsure about the decision or may have concerns. There are validated scales that measure attitudes related to safety, efficacy, past vaccine behavior and vaccine intentions.” said Limaye.
The CDC suggests providers ask vaccine-hesitant patients a scaled question, for example, “On a scale of 1 to 10, how likely are you to get the COVID vaccine? (1 = never and 10 = vaccine appointment is already set).” The goal is to help patients become more aware and move toward higher numbers on the scale.
For example, if a patient says that they are a three on the scale, providers can ask why and why not a lower number? This helps patients to reiterate the benefit of vaccines instead of explaining why they have not gotten it. Providers can then further follow up by asking, “What would help to go to a four or a five?”
While there are many successful ways to talk to people about the COVID vaccine — all methods center around a common theme of empathy, curiosity and open communication to help end the pandemic.
ABC News’ Sony Salzman contributed to this report.
Jess Dawson, M.D., a Master of Public Health candidate at Johns Hopkins Bloomberg School of Public Health, is a contributor to the ABC News Medical Unit.
(DALLAS) — Amanda Shoultz said she spent most of the past year trying to lose weight after noticing that her stomach kept getting bigger.
“I started working out more. I was dieting more and, oddly enough, I was losing weight but I was gaining inches in my stomach,” Shoultz, 29, told Good Morning America. “For the longest time, I thought, ‘Oh, I just must gain weight in my stomach.'”
When Shoultz, of Dallas, Texas, went to her annual checkup with her primary care physician in February, she said she was shocked at the number she saw on the scale.
“I remember telling her, ‘The next time you see me I’m going to be 10 pounds lighter,'” said Shoultz. “I just assumed it was my fault. That I had done something wrong.”
Shoultz’s blood work from her doctor’s appointment came back normal, so she said she kept changing her diet to see if she had an allergy that was causing her stomach to bloat.
“I gave up all dairy products because I thought it was a lactose allergy, and nothing changed. Then I gave up gluten. I love bread but I was willing to do anything,” she said. “That didn’t work so then I gave up meat. None of that helped.”
Shoultz said she did not feel any pain beyond the discomfort of her stomach getting so much bigger than usual.
By August, nearly eight months after first noticing the growth, Shoultz was referred to a gastroenterologist by a colleague at Baylor Scott & White Heart and Vascular Hospital, where she works in public relations.
“By the time I saw my GI [gastroenterologist] doctor, my stomach was hard as a rock,” she said. “My mom said you could have punched me in my stomach and broken your hand it was so hard.”
After several tests that did not find anything definitively wrong, Shoultz underwent a CT scan in late September.
“About four hours later, I got a call from my doctor who told me I had a 33-centimeter tumor in my abdomen,” she recalled. “And within two days of that, I was already meeting with the surgeon.”
Doctors discovered that Shoultz’s tumor was cancerous. She was diagnosed with liposarcoma, a rare form of tumor that, in most cases, does not present any symptoms until the tumor grows large and invades other organs or tissues, according to the National Institutes of Health (NIH).
In Shoultz’s case, the tumor had formed around her right kidney and adrenal gland, but she experienced no symptoms to indicate that cancer was growing inside her.
“I’m 29 and otherwise perfectly healthy,” she said. “I had no other symptoms other than my stomach.”
On Sept. 27, Shoultz underwent a two-hour surgery to remove the tumor, which doctors discovered upon removal weighed 17 pounds.
Doctors also had to remove Shoultz’s right kidney and part of her adrenal gland. Because the cancer had not spread to other parts of her body, she did not have to undergo further treatment, like chemotherapy or radiation.
“Once I left the hospital, my stomach was back to normal,” said Shoultz. “Now I’m just eating all the food that I missed when I gave it up for a year in order to put some weight back on.”
Shoultz said she is sharing her story publicly because she wants other people, particularly women, to know the importance of knowing and listening to their own bodies.
“I knew that something was wrong because I’ve always had a hard time gaining weight,” said Shoultz. “When I was getting so large in my abdomen and I couldn’t control it, that’s when I knew something was off.”
“We preach it at the hospital, don’t die of doubt,” she said. “No one else is going to need to fight for you, so fight for yourself and find a care team that is going to care for you through the journey.”
It’s a message echoed by Dr. Robert Mennel, an oncologist with Texas Oncology at Baylor University Medical Center in Dallas, who is treating Shoultz.
“There is a whole group of these sarcomas that tend to occur in younger people and a lot of times they have symptoms that are sort of very nondescript symptoms,” he said. “If somebody comes in and they have some abdominal discomfort and it’s somebody who’s in their 20s or so, most physicians think that’s probably not much and it will pass.”
“We can’t do scans on everybody, but if you really feel that something is wrong, just be persistent to get this evaluated,” added Mennel. “And make sure you’re going to somebody who has experience and really knows what they’re doing.”
“The takeaway would be that if you feel that something is not correct, see a physician or health care provider to let them evaluate it,” he said. “And if you really feel that they’re not evaluating it, or if you really feel that something’s wrong, pursue your desire to get it looked at and worked up.”
(NEW YORK) — The U.S. Food and Drug Administration has released sweeping new guidance for the food industry to voluntarily reduce sodium in processed, packaged and prepared foods in an attempt to reduce Americans’ consumption.
“The FDA is issuing a final guidance, ‘Voluntary Sodium Reduction Goals: Target Mean and Upper Bound Concentrations for Sodium in Commercially Processed, Packaged, and Prepared Foods,’ which provides voluntary short-term sodium reduction targets for food manufacturers, chain restaurants and foodservice operators for 163 categories of processed, packaged and prepared foods,” the agency announced.
Acting FDA Commissioner Dr. Janet Woodcock lauded the new sodium reduction guidance in a press conference Wednesday morning. She said it is a “critical step” in improving Americans’ nutrition, reducing the burden of diet-related chronic diseases and advancing health equity, predicting the effort would “become one of the most significant public health nutrition interventions in a generation.”
The guidance is intended to provide measurable voluntary short-term goals over the next two and a half years to reduce excess sodium intake, while recognizing and supporting the important roles sodium plays in food technology and food safety.
ABC News chief medical correspondent Dr. Jennifer Ashton said the news from Woodcock and Susan T. Mayne, director of the FDA’s Center for Food Safety and Applied Nutrition, is “really targeting the food industry.”
The current salt intake recommendation of 3,000 milligrams per day is now set to a goal of 2,300 milligrams a day over the next two and a half years.
“Right now, it is clear that diet is a major contributing factor to not only our obesity, but high blood pressure, which, of course, then increases the risk for heart attack [and] strokes,” Ashton said.
Woodcock voiced hope that this voluntary guidance that targets the food industry itself — rather than leaving the onus on individuals — will help level the playing field for Americans who may not be well-equipped to police their nutrition alone, especially with sparse healthy food options in food deserts and due to some healthier food options being cost-prohibitive for lower-income families.
“The problem is so cumulative — it’s the tomato sauce, the cheese, the bread, the salad dressing, and pretty soon your whole meal has hidden salt in it. And it’s really hard right now for people to manage that on their own,” Woodcock said. “Most of the salt in the diet, the sodium in the diet, it comes from processed or packaged or prepared foods — not from the saltshaker.”
“Sodium is widely present in the American diet (most commonly, but not exclusively, as a result of eating or drinking foods to which sodium chloride, commonly referred to as “salt,” has been added),” according to the FDA. “More than 70% of total sodium intake is from sodium added during food manufacturing and commercial food preparation.”
During the same press conference, Health and Human Services Secretary Xavier Becerra underscored Woodcock’s point that neglecting to address sodium consumption would carry high human and economic costs. He added that the COVID pandemic has shown the importance of taking better care of one’s health.
“The pandemic has graphically illustrated why today’s announcement is so important and why it’s so important that we take care of our health,” Becerra said, adding the consequences of Americans’ sky-high sodium intake could be “catastrophic personally and for the country.”
Mayne said that this issue impacts all age groups with “more than 95% of children age two to 13 who exceed recommended sodium limits for their age groups — even baby food — which carries long-term ramifications for children’s health and development,” she said.
But being that this is voluntary, truly capping sodium intake effectively will require a groundswell of both industry cooperation and consumer demand to help drive the initiative.
When asked whether there would need to be more teeth behind such policy, Woodcock said the government would monitor the impact of this current guidance over time, pointing to the importance of public support.
“If we don’t see success, then we’re going to have to evaluate what else we should do,” Woodcock said, without ruling out the idea of further, more stringent future measures.
“We have a plan to monitor and then to ratchet it further down, and what we learn over the next several years will tell us what magnitude of steps we can take,” Woodcock said. She acknowledged that “this change won’t happen overnight” and will require “an iterative approach that supports gradual reduction in sodium levels, broadly across the food supply, over time.”
(NEW YORK) — People with diabetes rely on blood glucose devices to monitor their blood sugar levels, but now people who do not have diabetes are tapping into the technology.
People without diabetes are using the devices, via apps, to learn more about how their lifestyle habits, like diet and exercise, may be affecting their blood sugar levels too.
One product designed for people without diabetes, Levels, features two sensors worn on the skin for 14 days each.
The product, currently in beta testing, links to an app that displays the user’s blood sugar level at all times so they can see how their body reacts to eating a bagel, for example, a food high in carbohydrates, versus a high-protein food like chicken.
ABC News’ Becky Worley, who did a complimentary tryout of the Levels app, found that while tracking her meals with the app, proteins like chicken and boiled eggs kept her blood sugar level, while a salad dressing loaded with sugar did not.
“What makes [continuous glucose monitors] so effective is that they empower people to learn about their health in a way that wasn’t possible before by seeing the impacts right away,” said Dr. Aaron Neinstein, a California-based endocrinologist who is not associated with Levels and prescribes continuous glucose monitors to his patients with diabetes. “I think what a lot of people learn when they use continuous glucose monitoring is just how much unhealthy ingredients are hidden in foods that we don’t know about.”
Medical experts say steady blood sugar levels generally keep the body in a state of using food as fuel, but big spikes in blood sugar can stimulate the body to store fat, increase your risk of heart disease and spur chronic inflammation.
Keeping blood sugar levels in range as much as possible can help delay or prevent health problems like heart disease, vision loss and kidney disease, and can help boost energy and mood, according to the U.S. Centers for Disease Control and Prevention (CDC).
Some of the keys to balancing blood sugar levels include avoiding processed foods, eating more protein, adding healthy fats like avocado, olive oil and nuts and even walking after big meals.
“When you’re exercising, your body is able to bring glucose or sugar into the cells without insulin,” Neinstein, also an associate professor in the University of California San Francisco division of endocrinology, told GMA. “So it is a very effective tool.”
While several continuous glucose monitors are approved by the Food and Drug Administration for use by people with diabetes, the Levels app is currently not FDA-regulated.
The company told ABC News that doctors routinely prescribe drugs and devices intended for other uses they think can help patients, but state in their terms of service, “We do not warrant that the results that may be obtained from the use of the service will be accurate or reliable.”
Neinstein said there is more data needed, stating, “Mu” h more research is needed to help us understand what the risks and benefits might be for people who don’t have diabetes.”
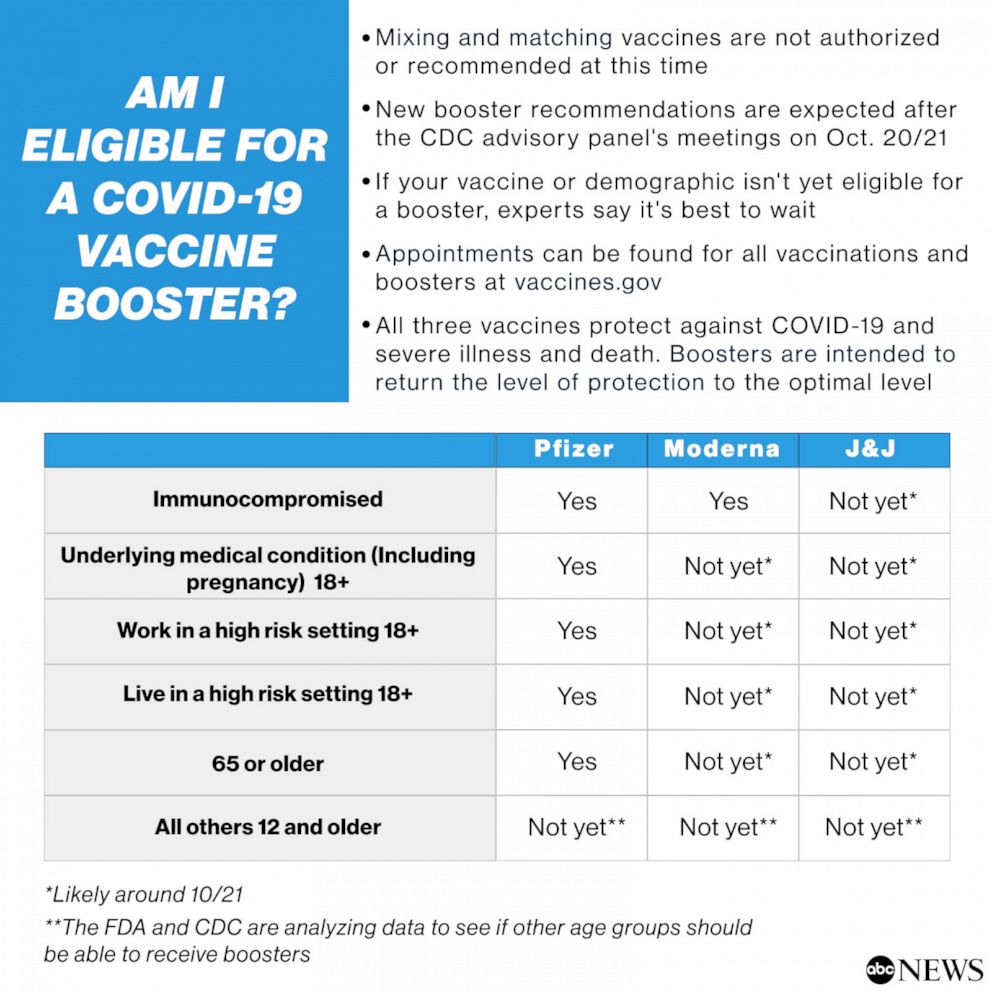
(WASHINGTON) — If it’s been six months or more since your second COVID-19 vaccine shot, you may be wondering whether you qualify for a booster.
In September, the Centers for Disease Control and Prevention endorsed an independent panel’s recommendation that older adults, along with those as young as 18 who have an underlying medical condition, receive a Pfizer booster shot.
CDC Director Rochelle Walensky also added a recommendation for a third dose for those in high-risk jobs or settings, such as nursing and teaching. Immunocompromised Americans, like those undergoing cancer treatment, have been able to get a third dose of the Moderna or Pfizer mRNA vaccines since mid-August.
But there has been a lot of public debate and there are different rules for Moderna, Johnson & Johnson, and Pfizer boosters, all of which can add to confusion. So, when is it your turn?
ABC News answers a wide variety of scenarios in the table below to let you know whether you qualify — and if you don’t today, when you might.
New booster recommendations are expected after the CDC advisory panel’s meetings on Oct. 20 and 21.
Boosters are intended to return the level of protection to the vaccine’s optimal level. Mixing and matching vaccines are not authorized or recommended at this time, but may be in the near future, and if your vaccine or demographic isn’t yet eligible for a booster, experts say it’s best to wait.
Appointments for all vaccines and boosters can be found at vaccines.gov.
(NEW YORK) — Infants born to mothers with COVID-19 are significantly more likely to experience health problems, such as difficulty breathing, compared to infants born to mothers without COVID-19, according to a new study published Monday.
The study, published in the Journal Of Maternal-Fetal And Neonatal Medicine, adds a new layer onto the growing body of research showing the potential complications COVID-19 can cause for both pregnant people and babies.
As COVID-19 continues to affect more expectant people in the United States, especially those who are unvaccinated, here are seven questions answered about pregnancy and the coronavirus.
1. Are pregnant people at higher risk?
Yes, pregnant people are at higher risk for complications from COVID-19.
Since the onset of the pandemic, more than 127,000 pregnant people have tested positive for COVID-19, 22,000 pregnant people have been hospitalized nationwide and at least 171 pregnant people have died as result of COVID-19, according to federal data.
COVID-19 causes a two-fold risk of admission into intensive care and a 70% increased risk of death for pregnant people, according to the Centers for Disease Control and Prevention (CDC).
Research published last month in the American Journal of Obstetrics and Gynecology, a medical journal, also found that pregnant people infected with the delta variant are more likely to have severe COVID-19 cases, and the variant leads to even worse outcomes for unvaccinated pregnant people.
2. What risks does COVID-19 bring to the fetus?
Pregnant people with COVID-19 are more likely to experience preterm birth, or delivering the baby earlier than 37 weeks, according to the CDC.
Poor pregnancy outcomes, such as pregnancy loss, have also been reported. There have been at least 266 pregnancy losses in the U.S. since the onset of the pandemic, according to federal data.
infants with COVID-positive mothers had two times greater odds of developing any type of adverse health complication during the birth process compared to infants with COVID-negative mothers, according to the research published in Journal Of Maternal-Fetal And Neonatal Medicine.
3. Is the COVID-19 vaccine safe for pregnant people?
Yes, the vaccines are safe for people who are pregnant, breastfeeding, trying to get pregnant or might become pregnant in the future, according to data compiled over the past nearly one year.
Both the Pfizer and Moderna vaccines use mRNA technology, which does not enter the nucleus of the cells and doesn’t alter the human DNA. Instead, it sends a genetic instruction manual that prompts cells to create proteins that look like the virus a way for the body to learn and develop defenses against future infection.
They are the first mRNA vaccines, which are theoretically safe during pregnancy, because they do not contain a live virus.
Messenger RNA vaccines for COVID-19, such as those produced by Moderna and Pfizer, showed no obvious safety concerns for pregnant women, according to a preliminary report published in April in the New England Journal of Medicine.
Messenger RNA, or mRNA, technology does not enter the nucleus of the cells and doesn’t alter the human DNA. Instead, it sends a genetic instruction manual that prompts cells to create proteins that look like the virus a way for the body to learn and develop defenses against future infection.
The Johnson & Johnson vaccine uses an inactivated adenovirus vector, Ad26, that cannot replicate. The Ad26 vector carries a piece of DNA with instructions to make the SARS-CoV-2 spike protein that triggers an immune response.
This same type of vaccine has been authorized for Ebola, and has been studied extensively for other illnesses — and for how it affects women who are pregnant or breastfeeding.
The CDC as well as the nation’s two leading health organizations focused on the care of pregnant people — American College of Obstetricians and Gynecologists (ACOG) and the Society for Maternal-Fetal Medicine (SMFM) — have all issued guidelines calling on all pregnant people to get vaccinated against COVID-19, citing the safety and efficacy of the vaccines.
The COVID-19 vaccines can be taken during any trimester.
Just 25% of pregnant people in the U.S. between the ages of 18 and 49 are currently vaccinated with at least one dose, according to the CDC.
4. What precautions should pregnant people take?
The most important thing pregnant people can do to protect themselves is to get vaccinated, and to make sure their loved ones are vaccinated too, medical experts say.
Pregnant people who are fully vaccinated should wear a face mask indoors when in public in areas of substantial or high transmission, avoid crowds and poorly ventilated indoor spaces and wash hands often with soap and water, according to the CDC.
Unvaccinated pregnant people should get vaccinated and continue masking until fully vaccinated, while also following safety guidelines like avoiding crowds and poorly ventilated indoor spaces, washing hands often with soap and water and staying six feet apart from people not in their households, according to the CDC.
5. Should pregnant people travel?
There is no guidance that pregnant people should not travel, so it’s ultimately a personal decision.
Pregnant people should consult with their doctors first. Factors to consider include where you’re considering traveling, how far along in your pregnancy you are and what your backup plan would be.
When traveling, pregnant people should wear a face mask that covers their nose and mouth.
In addition to considering whether the country in question has seen a significant influx of COVID-19 cases, think about the situation on ground. Has travel within the country been disrupted? How would you feel about potentially being quarantined upon returning to the United States? Is there a risk you could be grounded due to canceled flights or quarantines and not be able to travel home? Would you have access to medical care at your destination?
The U.S. State Department provides travel advisories that include up-to-date recommendations about which countries have reported cases of COVID-19 and how widespread infections have been. The situation is fluid and rapidly evolving, so you should check back often and use that information to inform what’s essentially a personal decision.
6. Can coronavirus be transferred to the fetus?
There is still more research to be done to determine whether a pregnant person could pass the virus to her fetus before, during or after delivery.
One small study in Italy last year found that a pregnant person infected with the coronavirus might be able to spread it to her fetus, but the study’s leader said it was still “too early to make guidelines” or to change care.
According to the CDC, some newborns have tested positive for COVID-19 shortly after birth but it is not known if the newborns got the virus before, during, or after birth.
7. Is it safe for a person with COVID-19 to breastfeed?
It is safe, in general, to breastfeed when you have COVID-19, according to both the CDC and the American College of Obstetricians and Gynecologists (ACOG).
The CDC recommends that people with COVID-19 wash their hands before breastfeeding and wear a mask when breastfeeding and whenever they are within six feet of the baby.
It is not likely that COVID-19 can pass through breast milk.
Recent studies have shown though that people who are vaccinated against COVID-19 may be able to pass along protection from the virus to their infant through breastfeeding.